

Chronic Total Occlusion (CTO)
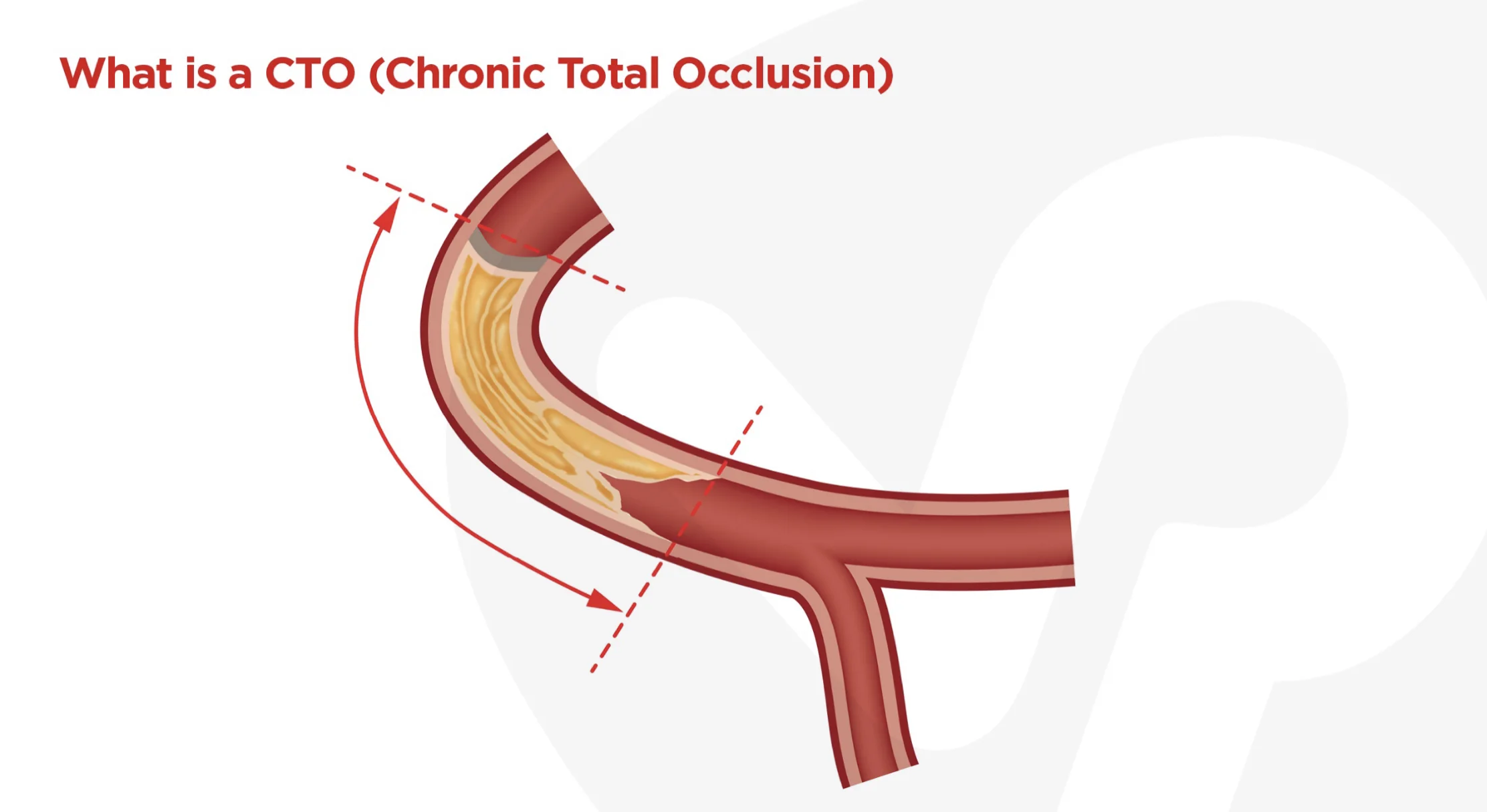

CHRONIC TOTAL OCCLUSION : final frontier in interventional cardiology
CTO PCI should only be performed if it carries a favorable risk/benefit ratio.
Benefits:
- angina relief
- improve exercise tolerance and left ventricular function
- improve tolerance of a future acute coronary syndrome
- reduce the need for coronary artery bypass graft surgery
- possibly improve survival if successful (especially for PCI of left anterior descending artery CTOs)
Pre-procedure planning & angiographic review:
- facilitates a thoughtful procedural approach and estimation of the risk–benefit ratio in this complex lesion/patient subset
- Understanding the vessel course and the presence, quality, and location of collateral vessels can allow rapid adjustments and change of strategies during the procedure and maximizes the likelihood of procedural success.

Approaches:
- Antegrade Wire Escalation (AWE)
- Antegrade Dissection Reentry (ADR)
- Retrograde Wire Escalation (RWE)
- Retrograde Dissection Reentry (RDR)
- hybrid approach: combination of ADR, AWE and RDR. Hybrid approach focuses on opening the occluded vessel, using all feasible techniques (antegrade, retrograde, true-to- true lumen crossing or re-entry) in the most safe, effective, and efficient way.


4 Angiographic characteristics dictate strategy:
1) clear understanding of location and morphology of the proximal cap using angiography or intravascular ultrasonography
2) lesion length
3) presence of branches, as well as size and quality of the target vessel at the distal cap
4) size and suitability of collaterals for retrograde techniques.
Safety considerations:
- Radiation exposure: use of collimation is the most effective way to reduce exposure to patients and operators. Rotate views to prevent radiation burns.
- contrast utilization
- procedure time
- Anaesthetic cover
CTO Approaches:
Antegrade Wire Escalation (AWE)
1. No proximal cap ambiguity
2. Lesion < 20mm
3. Good target
If clear path & target: Fielder XT➡️Confianza Pro 12
If unclear target & tortuous: Fielder XT ➡️ Pilot 200
Antegrade Dissection Reentry (ADR)
1. No proximal cap ambiguity
2. Lesion < 20mm
3. +/- Good target
4. Refractory
Dissection Reentry: CrossBoss
Reentry Method: Stingray
Retrogade Wire Escalation (RWE)
1. proximal cap ambiguity
2. Lesion < or = 20mm
3. Poor target
If clear path & target: Fielder XT➡️Confianza Pro 12
If unclear target & tortuous: Fielder XT ➡️ Pilot 200
Retrograde Dissection Reentry (RDR)
1. proximal cap ambiguity
2. Lesion < or =20mm
3. Poor target
4. Refractory
Dissection Reentry: Knuckle Wire
Reentry Method: Reverse CART












